Is scoliosis becoming more common as you age? The answer is “yes” in age degenerative scoliosis (ADS)
Research shows an increase in the number of geriatric diseases in aging populations around the globe. Specifically, there are more older people getting diagnosed with ADS. While scoliosis can be diagnosed as idiopathic, some research suggests that it is also due to hormonal changes during puberty, perimenopause/menopause.
An interesting find from a nurse out of Lurie’s Children’s Hospital in Chicago who went into business for herself specializing in bracing children and infants ~ Research findings at Lurie’s Children’s Hospital are suggesting it’s an autoimmune disorder. That research, however, is still being examined and investigated.
Some facts –
80% of females are affected by scoliosis vs 20% of men. Research also shows that neuromuscular diseases, osteoporosis, and sarcopenia increase the risk of getting adult degenerative scoliosis.
The causes of scoliosis – genetic utero, developed at puberty or menopause, or is secondary to a neuromuscular disease.
If you are starting to see the following:
- Your height changes aggressively in a short period
- You start leaning forward a lot or rounding your shoulder/back
- You notice one hip sticks out further than the other
- Your noticing leg length discrepancies
- Your lung capacity has decreased
- You feel like the bottom of your rib cage is hitting the top of your pelvis when you sit
- You can’t get comfortable and your spinal column hurts (or at least a portion of it)
- Because your shoulders and/or hips are asymmetrical, your clothes stop fitting properly • You often lose your balance
And if you notice any of this, schedule an Orthopedic doctor’s appointment. Within the Chicago market, Dr. Christopher DeWalk with Rush and Dr. David Manning with Northwestern (Head of Ortho @ Northwestern, will refer you out to the correct specialist within his practice) are highly recommended by my client base ~ I hear their names over and over. If you don’t live within the Chicagoland area, call these two resources, talk to the doctor’s nurse, and ask her who he would recommend in your area. You can also call Mayo Clinic’s Orth Div and ask for a referral.
Pls note: take heed with making sure the Ortho doc’s focused specialty is in fact scoliosis – this is definitely an expertise within itself. POV – don’t go to a shoulder Ortho or a Hip Ortho or even a knee Ortho – go to the big dog within the practice whose specialty is scoliosis. He/she will understand all the nuances involved in the changes going on within your structure.
Once you find an Ortho Specialist for Scoliosis, I highly recommend you insist on scheduling a full spinal scan – from the cervical spine through the tailbone. Often enough my client’s doctor only orders an x-ray of where the curvature seems most prevalent. But here’s the thing – what’s happening with your cervical spine (is your head tipped?) Your pelvis? Is one ASIS higher than the other? Why is one leg shorter (or seems to be) than the other? Does one hip swing out more than the other? When the pelvis is uneven and one femur is setting into the pelvis more securely than the other, the X-ray will give you this information. What about your tailbone? What is its shape?
Be your own advocate and insist on this and now you have a thorough depth of knowledge knowing what’s going on inside your physical structure. Pardon me – I can’t tell you how strongly I suggest a full body x-ray – cervical through the tailbone.
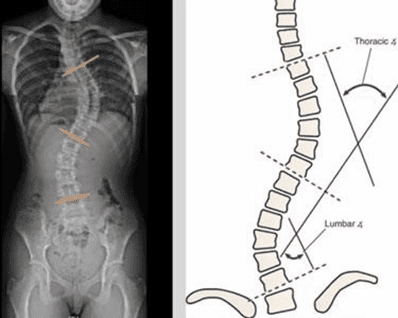
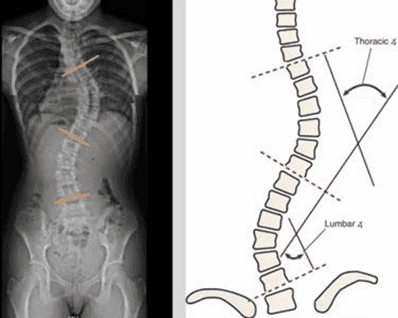
The medical testing diagnosis of scoliosis includes:
- X-ray imaging
- Cobb Angle Measurement: 20 degrees is considered mild; 20-50 degrees is considered; moderate. Above 50 degrees is considered severe scoliosis and fusion surgery is usually recommended.
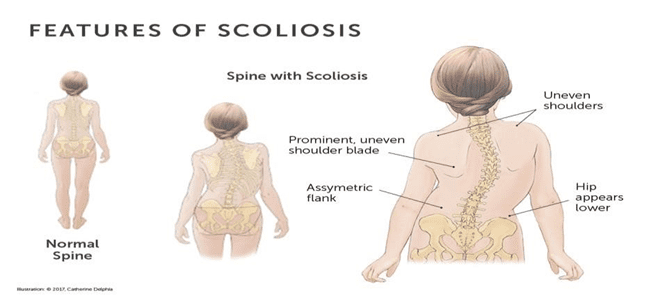
What exactly is Scoliosis?
A disorder of the spine causing:
- Lateral shifting of the spine
- A rotation of the vertebrae and ribs “s” or “c” shaped curve
There are two types of curves:
- Structural curve: misalignment of the bones (which can be managed and strengthened)
2-3% of the population have Structural Scoliosis, and an estimated 7-9 million in the US, or 1/10 persons are structural. With Structural Scoliosis, 75-85% are idiopathic, 10-15% are congenital scoliosis, and 10% secondary to a neuromuscular disease
- Functional curve: imbalance of the muscles (can be fully corrected permanently) 80-90% of the population have Functional. Functional scoliosis is a muscle imbalance and can be corrected. It is an imbalance of the bilateral muscle functioning of the back, without altering the bony structure. What’s its cause – repetitive habits that cause a lateral shift of the spine
- Holding a child on one hip, carrying a heavy bag on one side, poor postural habits, etc.
- Leg length discrepancy
- Can be reversed with yoga, Pilates, or other modalities
Let’s define vertebrae and the four natural curves
Your vertebrae are the small bones that make up your spinal column. These vertebrae stack on top of each other, separated by intervertebral discs. These bones protect your delicate spinal cord, which sends and receives information from your brain to the rest of your body. Your spine consists of 4 curves (cervical, thoracic, lumbar, sacral/coccyx) and 33 vertebrae – 7 cervical, 12 thoracic, 5 lumbar, 9 sacrum/coccyx – the sacrum/coccyx fuse at about the age of 26 to support the weight and structure of shoulders and hips.
Scoliosis will cause your vertebrae to move against each other more than they should. This can stretch and pinch your surrounding nerves, ligaments, and muscles, causing pain.
Muscles affected by the curvature(s)
- All Bilateral muscles in the body
- Intercostal muscles
- Diaphragm
- Erector Spinae muscles
- Latissimus Dorsi
- Trapezius muscle
- Rhomboid muscles
- Quadratus Lumborum muscles
- Iliopsoas muscles
- Core musculature
The characteristics of Scoliosis that no one probably ever told you (but now this makes sense)…
- Central Nervous system is overactive ~ sympathetic nervous system/fight or flight. Fun fact – the sympathetic nervous system lies in the thoracic spine. If your curvature is anywhere in the thoracic spine, your sympathetic nervous system is impacted. Why? Because the spine is trying to bring your head back to center so that it will sit correctly on the axis of the skull.
- Your balance is off
- Core/leg strength are highly affected
- Lung capacity is greatly affected, and breadth is shallow and uneven in the diaphragm/intercostal muscles
- You don’t know their center
- You tend to spasm easily – the spasming will be in the concavity.
- Prescription eyesight is different
Loren Fishman, MD is the medical director of Manhattan Physical Medicine and Rehabilitation in New York City, the author of eight books, and the author or editor of more than 70 academic articles. His research studies prove that yoga for scoliosis is an instrumental aid to those with scoliosis in utilizing the modality of yoga. The Serial Case Reporting Yoga for idiopathic and degenerative scoliosis is a very thorough research article he authored. And of course, I love his research on Yoga poses to reduce the curves in degenerative and adolescent idiopathic scoliosis.
At Dayton Children’s Hospital in Dayton, Ohio, Pilates for Scoliosis is part of the medical treatment plan for eligible patients with scoliosis.
I talk to new clients all the time who say to me “My doctor told me there is nothing I can do for my scoliosis. That can’t be further from the truth. My mission within this article is to improve, as much as possible, the lives of people living with scoliosis and raise advocacy and awareness.
A daily 10-minute (no less) Shivasan is imperative. My YouTube channel has over 50 free videos for you to refer to as a resource choice and learning of lengthening, derotating, and strengthening your curvatures. No matter what the curve in your back looks like, it’s imperative to focus on building strength and improving your posture through the modalities of Yoga for Scoliosis and Pilates for
Scoliosis. After all, we always feel better when we come move more freely and be out of pain.
What should your overall weekly practice consist of – it has to be this formula to see positive changes:
- myofascial release – you can’t move the bones into their proper structure unless this is practiced. A massage would do the same thing.
- joint mobility (the muscle can only strengthen fully if the joint is mobile and in alignment).
- understanding the learning of hugging the curvature into the midline, lengthening out of the concavities, and derotating the curve pattern(s) thru ScolioYoga and then keeping all of this correction within the structure,
- to strengthen the muscle group just lengthened thru Pilates for Scoliosis or Reformer for Scoliosis
- encompass a practice of rewiring the brain in specific pranayams and shivasans.
The challenge is that – you have to do the work. If you don’t have a home discipline, nothing will decrease (or at least halt) your curvature. It could be as simple as 5 minutes daily plus a 10-minute Shivasan daily. Why is the shavasana imperative? It rewires the brain AND calms the sympathetic nervous system. An added bonus to this is from staying in the posture for a 10-minute segment, in a short period of time, you will find your shoulders and pelvis more square. Many of my clients state that this simple posture has totally relieved their lower back pain because their pelvis becomes more symmetric.
About the author ~
Linda Benton is a Certified Yoga Therapist and Certified Scoliosis and Back Care specialist and President of ScolioYoga, LLC. She holds over 20 years of experience in teaching Yoga and Pilates. As a Certified Yoga Therapist for Scoliosis, Advanced Pilates for Scoliosis and Reformer Certified, she customizes 1:1 sessions (virtual or in studio) to teach you a home practice to make you Scoliosis STRONG thru, therapeutic movements and techniques utilizing the modalities of Yoga and Pilates for Scoliosis.